Lessons from the Field
New Incentives’ Approach to Treating Childhood Diarrhea

In February, New Incentives received exciting news: GiveWell recommended a grant of up to $4.8 million to provide oral rehydration solution and zinc supplementation (ORSZ) for babies enrolled in their program in Nigeria (read more). This grant will enable caregivers to treat childhood diarrhea, a leading cause of death in children under five in Nigeria, responsible for 100,000 lives lost each year (source). As they embark on this critical work, they're sharing some of the lessons they've learned and the refinements they're making to their approach.
Defining Diarrhea: A Complex Task
Understanding the definition of diarrhea and ensuring caregivers grasp this definition is not as simple as it sounds. According to the WHO, diarrhea is defined as the passage of three or more loose or liquid stools per day. Misconceptions around the identification of diarrhea are deeply embedded in society at large. For instance, in the US, it’s common for parents to mistake one loose stool as diarrhea in their child.
New Incentives held informal focus groups in multiple locations in northern Nigeria to learn more about caregivers' perceptions of diarrhea in their children and their understanding of the data collection questions about diarrhea incidence we crafted in collaboration with our research partner IDinsight. They discovered two common misconceptions about diarrhea. Caregivers sometimes believe that teething causes diarrhea and thus doesn’t need to be treated. They also learned that caregivers believed the color of the stool was important in identifying when their child was suffering from diarrhea.
These observations changed how New Incentives ask questions about diarrhea and educate caregivers on proper identification so they can treat their children.
Fine-Tuning Caregiver Education
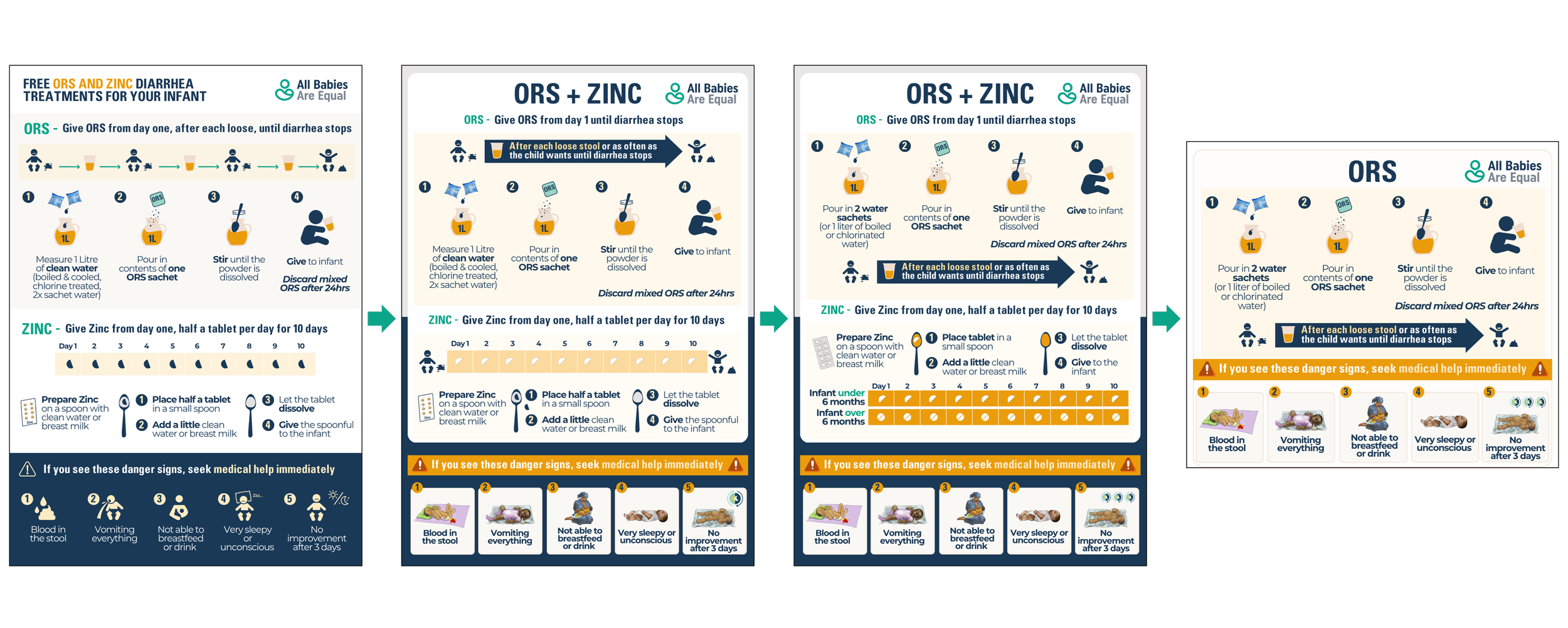
Though New Incentives designed their own informational flyer to provide to caregivers along with the ORS and zinc, they used flyers by Clinton Health Access Initiative (CHAI) and Clear Solutions as a starting point. They then iterated multiple times after getting feedback from field staff, assessing gaps in caregiver knowledge upon probing, and stakeholder suggestions. Here, you can see a progression of flyer designs.
When it comes to proper preparation and administration, they’ve learned a lot.
Some clinic staff expressed concern surrounding providing ORS proactively (as a take-home package) to caregivers of very young infants who may not currently have diarrhea. They worry that this could confuse caregivers who are being told to practice exclusive breastfeeding and not give any other liquids unless medically necessary. New Incentives plan to address this in staff training to reinforce messaging about exclusive breastfeeding alongside only giving ORS when the child is sick.
Metric units of measurement, such as litres, are not familiar or easily understood by caregivers in northern Nigeria. Because of this, New Incentives are focusing on explaining the preparation of ORS using water sachets. These sachets are plastic bags of water that come in 500ml size and are readily available throughout urban and rural areas. They are also a safe source of water, which is another vitally important element of preparing ORS.
They found confusion among field officers and caregivers regarding when to start giving ORS. Some understood that it should be given after the first time the child has a loose/watery stool; in staff trainings and knowledge tests of caregivers, we now emphasize that ORS should begin after the third loose stool, as ORS is given once a child has diarrhea (three loose or watery stools in 24 hours).
The Zinc Conundrum
New Incentives has been grappling with whether to include zinc in their treatment protocol ever since they understood that zinc does not have mortality benefits (and minimal morbidity benefits). Yet zinc accounts for ⅓ of the cost of a co-pack (2 ORS sachets and 10 zinc tablets). This led us them dig deeper into the literature, thoughts from other implementers, and feedback from Nigerian state health officials.
ORS and zinc, individually and co-packaged together, are recommended by WHO for the treatment of diarrhea (source). New Incentives learned that some actors in Nigeria distribute co-packs of ORS and zinc to caregivers, while others distribute ORS only. There are many open questions around the benefit of zinc in potentially providing medicinal value and increasing the uptake of ORS. There are also questions surrounding adherence, as children are supposed to take zinc once daily for 10 days, even after they recover.
When they reviewed the literature, New Incentives found that there is strong evidence that zinc reduces the severity and duration of diarrhea in older children, yet there is also statistically significant heterogeneity in studies that include only children under 12 months (source)—New Incentives’ target population of babies who are eligible to receive ORS. The evidence regarding zinc’s effects on mortality is weak and limited (source). Though of more minor concern, they still have questions regarding the risk of vomiting and the effectiveness of zinc based on the cause of the diarrhea and the type of zinc supplement administered.
New Incentives also spoke with a pediatric nurse practitioner in the United States who noted that, in her experience, providing multiple simultaneous treatments can sometimes be confusing, particularly when literacy levels vary. While anecdotal, they think this lesson may translate to their context. With their model, we provide detailed instructions on the preparation and administration of two different interventions given for the same purpose. It’s possible that caregivers could mix up ORS and zinc and think the zinc is given after each loose stool and the ORS is given once a day. That would worsen dehydration, considering zinc’s side effects of vomiting with a regular dose. Caregivers may not even use it for weeks (or maybe months). This lapse in time presents additional challenges for caregivers to remember and administer correctly.
For now, New Incentives will be distributing ORS only. They hope to leverage these cost savings by providing more ORS to infants, as this simple intervention can reduce diarrhea-related child deaths by up to 93% (source). They are very open to adding zinc later if the evidence surrounding its effectiveness in younger children (under one) and its effect on reducing mortality becomes more robust.

ORS Packaging: A Barrier to Better Treatment
In Nigeria, ORS packaging comes in 20.5g sachets. The dry powder is then reconstituted with 1 litre of water. This works well for a hospital or clinic setting, which often prepares ORS to treat multiple children throughout the day. But for household use, this volume poses an issue, as whatever remains at the 24-hour mark must be discarded to avoid contamination.
A young child doesn’t consume a liter’s worth of ORS on their own in 24 hours. This is challenging. Based on caregiver feedback, New Incentives think that caregivers aren’t always discarding ORS after 24 hours and that they may be trying to mix smaller batches by only using half of a sachet at a time, but this may cause dilution issues.
They aren’t the first to recognize this. Other implementing partners in Nigeria lament this too—but the quantities they procure don’t provide the leverage needed to shape the market and, therefore, the packaging. ColaLife was an organization that advocated for decreased sachet sizes and made headway toward this goal in Zambia.
New Incentives goal is to procure ORS sachets that are half the size (10.25g) and can be reconstituted with .5 liters of water (or one water sachet). They are already making progress and working with a pharmaceutical manufacturing company to do this. They hope that this will reduce waste and increase adherence to preparation and administration.
These lessons highlight the importance of continuous iteration and adaptation in our program. New Incentives are committed to refining their approach based on data and feedback, ensuring that their intervention is cost-effective, evidence-based, and impactful. They’re committed to ongoing learning and improvement, and hope that their experiences will contribute to the broader conversation on effective diarrhea treatment in low-resource settings.